Due to the staggering rise in cases of the highly transmissible B.1.1.529 (Omicron) variant of SARS-CoV-2, the virus that causes COVID-19, demand for testing surged — but testing capacity became a bottleneck in the nation’s COVID-19 response. Home tests are still difficult to find at most retailers, many testing sites have long lines or limited appointments, and turnaround times for results may be protracted due to backlogs. Although the federal government has launched a national home delivery program for antigen tests, many county and local municipalities must still identify creative solutions for managing testing demand in both the short- and long-term.
Healthy Davis Together (HDT), a joint project between the University of California Davis (UCD) and the City of Davis, provides quick, convenient, and community-wide saliva-based COVID-19 testing. HDT uses a high-throughput, low-cost testing platform developed by the UC Davis Genome Center to process its samples, which are collected at a number of testing locations across the county. Affiliated testing locations have included five community testing sites, school testing sites at five separate K–12 school districts, and a mobile team that reaches underserved locations across Yolo County.
Since launching its testing operation in late 2020, HDT has been able to successfully and responsively adjust its scale to meet testing demand. This flexibility was demonstrated recently when plans to reduce the scale of HDT’s testing operation beginning in January 2022 were quickly adjusted to respond to the spread of Omicron and allow HDT to retain high testing capacity and improve access where necessary. Since late-December, HDT has collected a weekly average of roughly 24,000 tests — significantly higher than its prior weekly average of 16,000 — with results continuing to be returned within an average of 24 hours.
Ensuring flexibility to meet testing demand is crucial to the success of mass testing initiatives. As we continue to respond to the dynamic nature of this pandemic, HDT has identified four key practices that have enabled it to quickly calibrate its testing program. These practices and recommendations can help other communities improve their testing responsiveness and flexibility:
- Establish a network of temporary staff: Creating flexibility with human resources is critical for meeting fluctuating testing demand. The core staff for HDT were hired as university employees. To expand the program in times of need, HDT draws from a network of other staff sources that include:
- Staffing overflow from other organizations or departments: HDT partnered with the county Health and Human Services Agency to mobilize available disaster response workers. HDT was also successful in pulling in staff from departments at UC Davis that experienced a decrease in staffing needs during the pandemic (e.g. catering). Contacting organizations that had recent lay-offs or furloughs may help identify available staff looking for work.
- Staffing agencies: Staffing agencies can help with legwork and may have greater contract flexibility (e.g., shorter notice requirements) to meet short-term demands.
- Part-time students: Through UC Davis, HDT had the benefit of an engaged university student body. Contacting students and relevant university programs at local colleges (public health/nursing undergraduates and graduate students) may draw in passionate individuals who are looking for relevant experience and opportunities to learn about public health.
- Parent volunteers: HDT has begun recruiting and training parent volunteers. Depending on the testing model (saliva vs. nasal), parents of K–12 students may be mobilized to collect samples on school sites on a volunteer-basis. HDT has developed a step-by-step guide for testing on school sites here.
- Increase existing testing site throughput: Implementing process efficiencies can increase throughput at testing sites. When wait times were high at testing locations, HDT tried several adjustments to improve processing speed and productivity including:
- Assessing and reassessing sites for potential bottlenecks. For example, greeters stationed at the entrances of testing site parking lots created traffic slowdowns, and moving greeters to the front door of the testing site allowed for a more streamlined flow of testers.
- Changing the flow of people seeking testing from one single line to two lines. One line for those who made appointments (priority line) and the other for walk-ins. An additional option to consider is transitioning to by-appointment only at times of high demand.
- Transitioning staff from working one saliva testing station to working up to three stations, shifting between the stations to provide instructions and collect completed samples. Note that this efficiency is applicable only to staff-monitored self-administered testing.
- Encouraging teachers at K–12 school district sites to bring their full classes to the on-site testing location and run through the process in roll-call fashion. This process became very familiar to Davis students of all ages and reduced time to test by as much as 66% compared with individual testing. A diagram of this process along with the steps for replicating it are included at the end.
- Identify new testing site locations: Existing testing site space may limit the number of registration/check-in and sample collection stations due to social distancing guidance. HDT worked with local government, community organizations, and current site providers to identify vacant or available community spaces (indoor or outdoor) that could be quickly converted into temporary testing sites. Options included community meeting rooms/event venues, veterans’ centers, libraries, city halls, and much more. For both public and private event spaces, HDT worked with organizations to identify test site times that fit into their event schedules.
- Clearly communicating testing guidelines and availability: Clear and consistent messaging about guidelines on what kind of test to get and when to get tested — such as how long after exposure or symptom development — are essential. HDT and local health officials communicated testing guidance to the community on the appropriate times to test (e.g., after exposure, in response to symptoms, or before necessary gatherings) and promoted HDT testing location as well as alternative testing options (e.g., local pharmacies, primary care providers, home test vendors). Regular updates to a centralized and accessible testing information source, like HDT’s website, is also crucial for providing accessible up-to-date guidance as well as public insights into the prevalence of the virus and the current demand for testing.
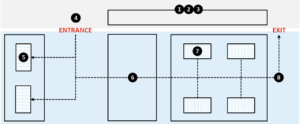
Example School Testing Flow
The following outlines a streamlined method of conducting class-by-class school testing*:
- Teacher brings class just outside of the testing area on-site during a defined time slot
- Greeter orders students alphabetically using roster, separates out registered vs. non-registered students, and hands each registered student a notecard with their name and grade
- Teacher takes non-registered students aside and sits with them while registered students test
- Greeter directs students to registration/check-in station as available
- Check-in/registration personnel confirms student name and grade (and takes notecard), provides ‘boat’ of testing materials, and assigns student to sample collection booth (if available) or waiting area (if occupied)
- [If waiting] Student stands on designated social-distancing marker in waiting area
- Sample collector calls next student in line and walks through sample collection process
- Sample collector directs student to exit and sit with teacher and classmates
*This information is meant to be a general guideline, but it is not intended to be medical or clinical advice; the licensed Provider Partner operating the sample collection site should provide all clinical and medical standard of care decisions
